 Blog")
Exeter Collaboration for Academic Primary Care (APEx) Blog
Exeter Collaboration for Academic Primary Care (APEx) Blog
Posted by ma403
8 July 2026Eleanor Dunstan and Lianne Wood on behalf of the author team.
This is a summary blog of the paper accepted in the EMJ: Dunstan et al., Same day emergency care for low back pain: quality improvement to support emergency flow and reduce unnecessary acute admissions https://tinyurl.com/35e2367s .
Low back pain (LBP) is one of the most common reasons for emergency department (ED) attendance, yet most patients do not require hospital admission. Despite this, admission rates remain high, placing pressure on already stretched services and exposing patients to low-value care.
In our recent quality improvement project at Nottingham University Hospitals, we set out to address this challenge by redesigning how LBP is managed at the ED–spinal interface. The result was the development and embedding of a same day emergency care (SDEC) pathway, delivered by a specialist multidisciplinary team and led by advanced practice physiotherapists (APPs).
What did we do?
We repurposed a 12‑bedded unit adjacent to the spinal wards, creating a dedicated SDEC unit for patients with non-traumatic spinal pain. The service was co-designed with ED clinicians, spinal surgeons, radiology and patients, ensuring it met both clinical and operational needs.
Key features included:
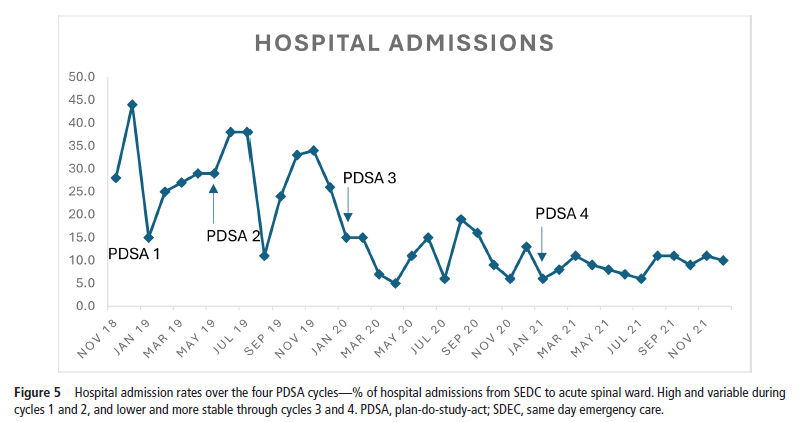
The pathway was developed iteratively over four plan–do–study–act (PDSA) cycles, allowing ongoing refinement based on real-world feedback and data.
What were the outcomes?
Over three years, we saw more than 3,900 referrals to the SDEC pathway. As the service matured, several key improvements emerged:
Importantly, these improvements were progressive and sustained, reflecting both increased system engagement and optimisation of the pathway over time.
Why did it work?
Several factors were critical to success:
Senior clinical decision-making
APPs, with their expertise in musculoskeletal care and biopsychosocial management, were well positioned to provide supportive reassurance, holistic care and discharge decisions with support from the spinal on call team to avoid unnecessary admission.
Whole-system collaboration
The pathway was not an ED initiative alone—it relied on strong partnerships between ED, spinal services, radiology and primary care. An ED–spinal interface group was key to maintaining alignment.
Iterative improvement
Using PDSA cycles allowed us to identify barriers early (e.g. low referrals, inconsistent handovers) and adapt rapidly—whether through education, process redesign or workforce changes.
Focus on flow, not just care delivery
By creating a dedicated pathway outside the ED, we improved both patient experience and departmental flow, aligning with broader SDEC principles of delivering “right care, right place, right time”.
What should other services consider?
For clinicians and healthcare leaders looking to implement a similar model, a few key lessons stand out:
Final thoughts
Our findings suggest that a spinal SDEC pathway is a feasible and effective alternative to traditional ED pathways for patients with non-traumatic LBP. While further work is needed to evaluate cost-effectiveness and long-term outcomes, this model offers a practical way to reduce unnecessary admissions and improve system efficiency.
At a time of increasing demand on ED services, rethinking pathways for common conditions like LBP presents a real opportunity for meaningful transformation.
