
Haemochromatosis: genetic iron overload disease
Summary for patients
Haemochromatosis: genetic iron overload disease
Summary for patients
You have two copies of the HFE C282Y genetic variant.
* Estimates are from our community sample of UK Biobank European descent individuals [1]. People tested because of a health problem or with high iron levels may have different risk. See below Technical Details section for more information, and the Risk Modifiers page. Page updated 25th May 2023.
Males are known to have higher risk of iron overload disease compared to females.
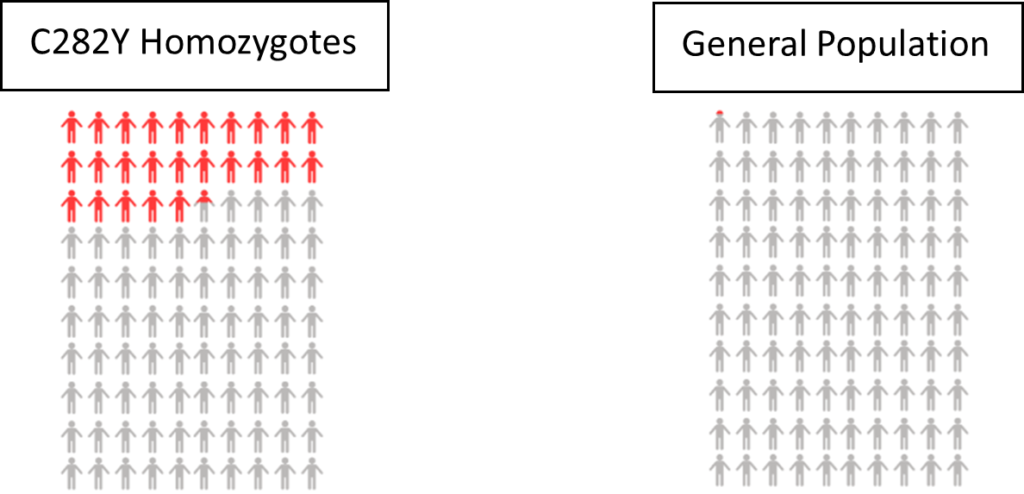
Haemochromatosis – 25.3% of men in our study with two copies of the HFE C282Y gene variant were diagnosed with haemochromatosis. In comparison, only 0.06% of men without a faulty HFE gene were diagnosed. Data from the UK Biobank participants linked medical records up to Jan 2018 [1].
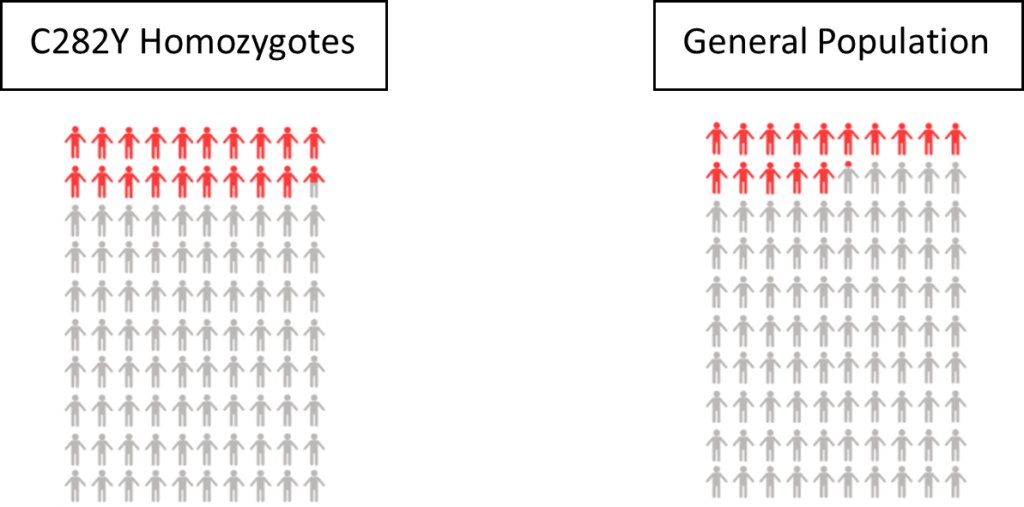
Mortality – We estimated that 19.5% of UK Biobank males with two copies of HFE C282Y would die by age 75, compared to 15.1% of individuals with no faulty HFE genes.
Liver cancer – Male C282Y homozygotes were more likely to be diagnosed with liver cancer by age 75 than men without faulty HFE variants (7.2% vs. 0.6%).
Liver disease – 22.7% of male C282Y homozygotes were diagnosed with liver disease (non-cancer related) by age 75, compared to only 10.2% of men without either HFE variant.
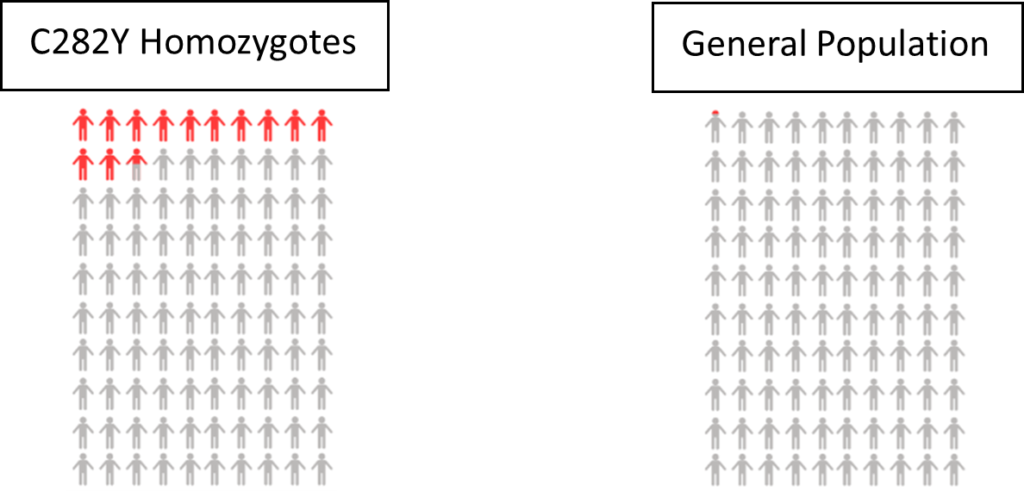
Haemochromatosis – 12.5% of women with two copies of the HFE C282Y gene variant were diagnosed with iron overload-related haemochromatosis. In comparison, only 0.02% of women without a faulty HFE gene were diagnosed.
Risk of disease/mortality – In our study of mortality and disease risk to age 75 in UK Biobank, females with two copies of the HFE C282Y gene variant did not have increased risk of death or liver complications (including liver disease and liver cancer).
The UK NHS website for haemochromatosis (link) says to speak to your GP about getting a test if:
Because you have two copies of HFE C282Y you are at higher risk of haemochromatosis than the general population, and should therefore consider talking to your GP even if you do not currently have symptoms.
1. See below effect estimates for disease and mortality for male and female C282Y homozygotes:
2. Genetic differences among different populations can influence the risk of disease prevalence and rates of mortality. Therefore, the generalisability of our study findings may be limited to individuals of European descent.
3. Early follow-up years are liable to be impacted by healthy volunteer bias in the UK Biobank. However, the present study’s findings reported incident outcomes with sufficient follow-up time (median of 8.9 years), thus, limiting the influence of a healthy volunteer bias.
4. The current study does not take into account other genotypes that are known to influence iron metabolism. Therefore, the potential implication of such modifiable effects on iron could have affected any associated risks of disease or mortality. However, further research is required to determine the extent of such effects.
5. We determined C282Y genotype status through imputation; however, when comparing this with sequencing data in a subset, we found only one C282Y homozygotic participant to be misclassified as a C282Y heterozygote. Thus, there was a minor impact on the attenuation of excess risks associated with the homozygote genotype.
6. Although our study had an adequate duration of follow-up, the incidences of our studied health outcomes were limited, thus, affecting the statistical power of our reporting capabilities. For example, we observed only one liver cancer diagnosis among female individuals with the C282Y homozygous genotype.
[1] Atkins et al. (2021) “Association of Hemochromatosis HFE p.C282Y Homozygosity With Hepatic Malignancy” JAMA. doi:10.1001/jama.2020.21566
[2] UK NHS Haemochromatosis overview – https://www.nhs.uk/conditions/haemochromatosis/